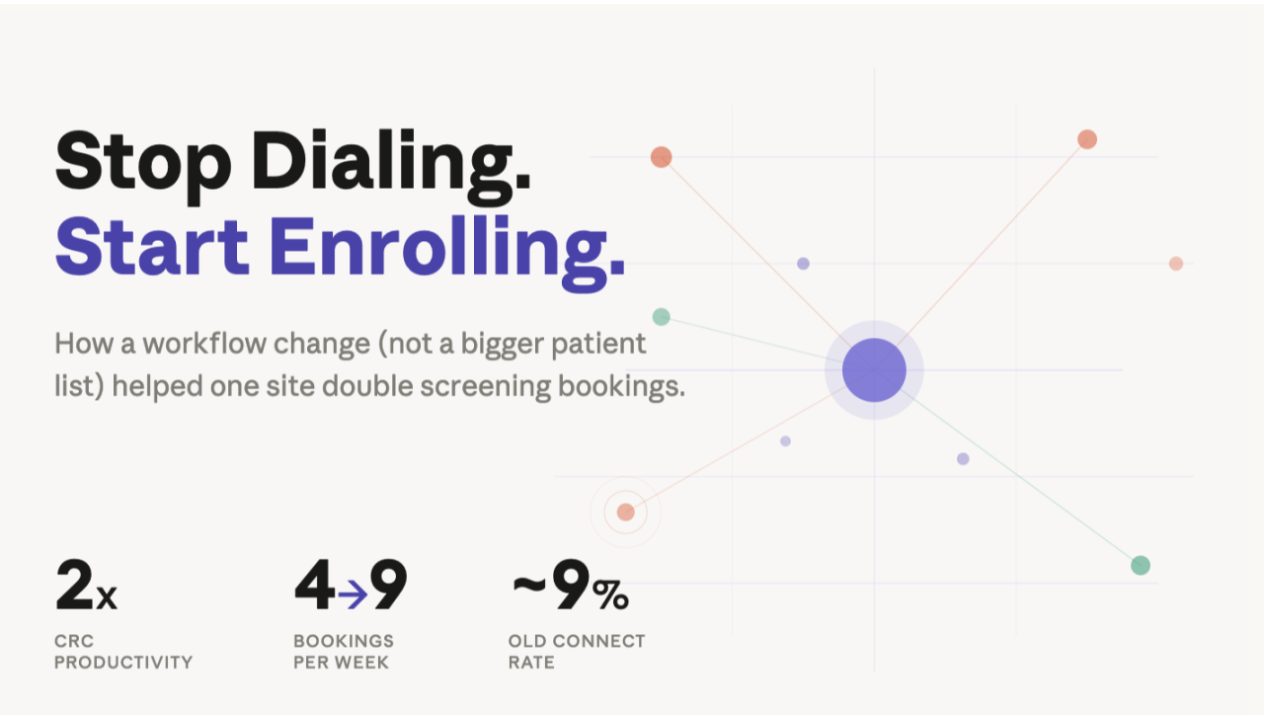
How a workflow change (not a bigger patient list) has already helped one site double their booking visits.
A CRC at one of our partner sites doubled her weekly screening visit bookings in two weeks. Went from 4 to 9. She didn't hire anyone. She didn't change her protocol. She didn't get a bigger patient list.
She stopped manually dialing.
That sounds like a punchline, but it's pointing to something we think most ops teams are overlooking: the referral to screening visits booked gap often isn't a sourcing problem. It's a calling problem.
What's Actually Happening at Your Sites Right Now
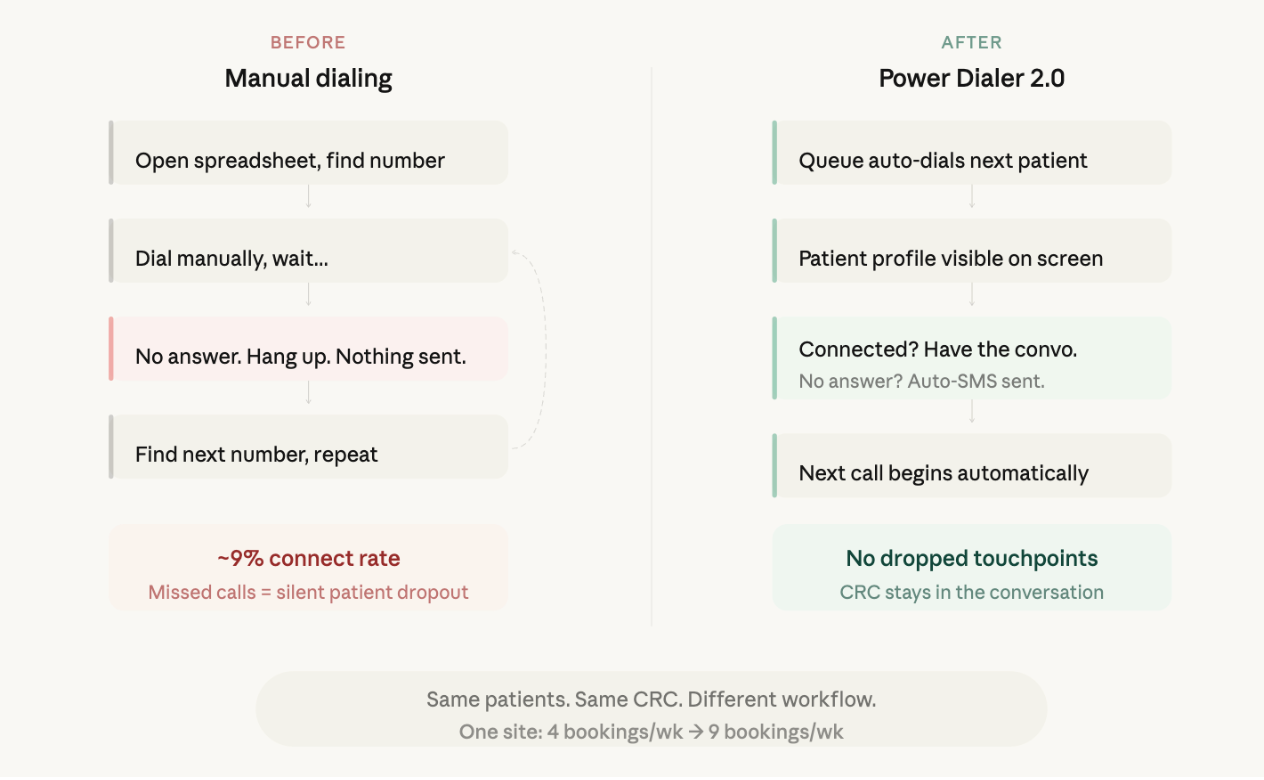
You probably already know this rhythm. Open the spreadsheet (or site portal). Find the next number. Dial. Wait. No answer. Hang up. Find the next number. Repeat.
At most sites, this eats 2-3 hours of a coordinator's day, and the connect rate on outbound calls tends to sit in the single digits (across the board: cold-call benchmarking sits at 5-10% pickup rate).
But the answer rate isn't the real issue. The real issue is what happens after the missed call.
When a patient doesn't pick up and there's no follow-up, that's often the end of the story. Not because they lost interest, but because the window closed. We dug into this in our survey of 1,000+ patients, and the numbers were stark: 54% of patient contacts ended in some version of "we'll talk later." Only 17% left their first site interaction with a screening visit on the calendar.
A missed call with no follow-up isn't just a gap in your outreach. For many patients, it's the moment they quietly exit your funnel — and this is often overlooked.
The Mismatch
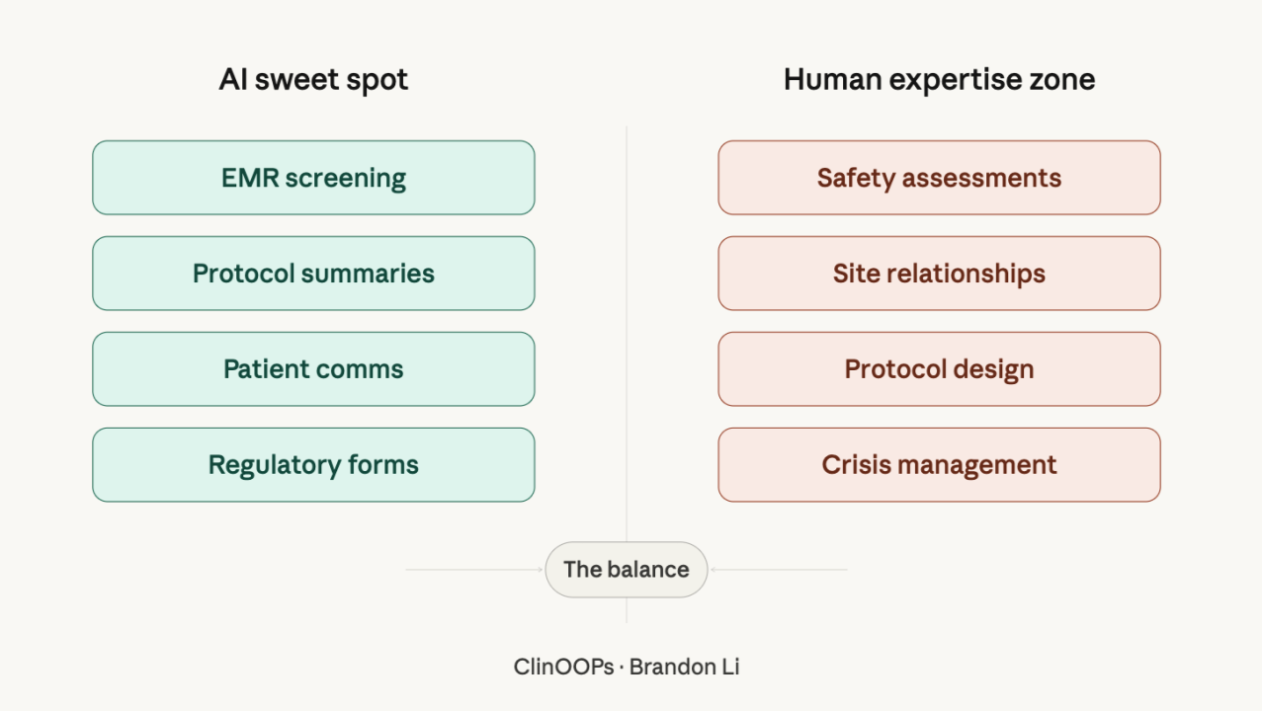
Here's the thing that keeps bugging me about this: CRCs are trained clinical professionals. They understand medical histories, eligibility criteria, protocol nuances. They know how to build rapport with an anxious patient in a 3-minute phone window. The CRCs who convert patients at the highest rates are the ones who can review a profile, anticipate questions, and meet someone where they are emotionally.
It makes it more difficult to focus on that when fumbling between tabs to find the next phone number.
So we rebuilt our dialer from the ground up.
What We Changed
Power Dialer 2.0 replaces the manual, one-at-a-time workflow with an intelligent queue. When one call ends, the next begins automatically. The CRC sees the patient's full profile on screen during the call: medical summary, medications, birthday, eligibility flags. When a patient doesn't answer, the system sends a follow-up text automatically (customizable by the coordinator, not some generic template). Conversation detection filters out voicemail so coordinators aren't wasting time talking to machines.
What the Happy Path Actually Looks Like
So what does this feel like for a coordinator when it's working?
The CRC logs in, hits start, and the queue takes over. Power Dialer 2.0 begins calling through their patient list automatically, in priority order. There's no dialing, no searching for the next number, no switching between tabs. One click, and the conversations come to them.
When a patient picks up, the CRC is already looking at their full profile: diagnosis, current medications, eligibility flags, previous interactions. They're not scrambling to pull context mid-sentence. They're having a real clinical conversation from the first word.
When a patient doesn't pick up, the system detects it (conversation detection distinguishes a live human from voicemail) and automatically fires off a personalized follow-up SMS the coordinator has pre-written. No dropped touchpoint. No hoping the patient calls back on their own. The dialer moves to the next patient immediately.
Between calls, coordinators can set a pause timer to review the next patient's profile before the ring goes out. It's a small feature, but CRCs told us it matters: that 15-second window to scan a medical history is the difference between a cold call and a warm conversation.
And here's a detail that surprised us operationally: when a patient calls back inbound while a session is running, that call gets organized into the queue rather than interrupting whatever conversation the CRC is in the middle of. No more fumbling between an active call and an inbound ring. Everything flows through one interface.
The result is closer to what you'd want: when a dial connects, it's a conversation with a prepared coordinator. No wasted calls. No wasted CRC time. Just conversations.
What Surprised Us
Two weeks post-launch, we expected a gradual adoption curve. Sites easing in, testing it on a few calls, ramping up over time.
That's not what happened.
CRCs have now over 2X'd their baseline productivity.
Also, sites that tried it didn't dabble. They switched. We have only rolled it out to ~20% of sites, with a gradual rollout to all sites expected in the coming months.
Here's what they're telling us:
A Florida CRC, with refreshing honesty: "I used it today and I actually really like it. I was like, okay, I actually like it." (If you've collected site feedback before, you know that surprised enthusiasm from a busy coordinator is worth more than any polished testimonial.)
A New York coordinator on the patient profile view: "I love the info update... their medications, their birthday. I like reviewing it before I speak with them."
And one detail from our feedback sessions that stuck with me: a coordinator at one of our initial rollout sites told us she couldn't fully adopt the tool until the auto-SMS on missed calls was live. Not because the dialer wasn't useful, but because she refused to let a single patient go uncontacted. If the system couldn't guarantee a follow-up on every missed call, she wouldn't use it.
That's the CRC mindset. These aren't people looking for shortcuts. They care about every touchpoint, and they need tools that match that standard.
So What?
I want to be upfront: two weeks of early data is not a controlled study. One site doubling bookings is encouraging, but it's a single data point in a small window.
What I'm more confident about is this: the manual calling workflow that wastes coordinator expertise and creates silent dropout events is a real, widespread problem that most ops teams aren't examining closely enough. When you audit enrollment performance, you tend to look at referral volume, screen fail rates, activation timelines. You rarely look at what's happening inside the calling workflow itself.
A few questions worth bringing to your next team meeting, regardless of what tools your sites use:
What happens after a missed call? Is there a systematic follow-up, or does it depend on whether the coordinator remembers to circle back?
How much of your coordinators' day is spent on the mechanical act of dialing versus the clinical act of engaging patients?
These tend to surface uncomfortable answers. Which is usually a sign they're the right questions to ask.
The pattern we keep seeing — across this launch, across our Silent Dropout data, across hundreds of site interactions — is the same: trials don't stall because patients aren't out there. They stall because the space between "patient expressed interest" and "patient showed up" is full of small, fixable friction points that compound silently.
Stop dialing. Start enrolling. More to come!
Brandon Li · Co-Founder, Power
For clinical operations teams thinking through enrollment workflows: Talk to our team about what we're learning across our site network.