Why the gap between 'interested patient' and 'scheduled screening' is costing you enrollment
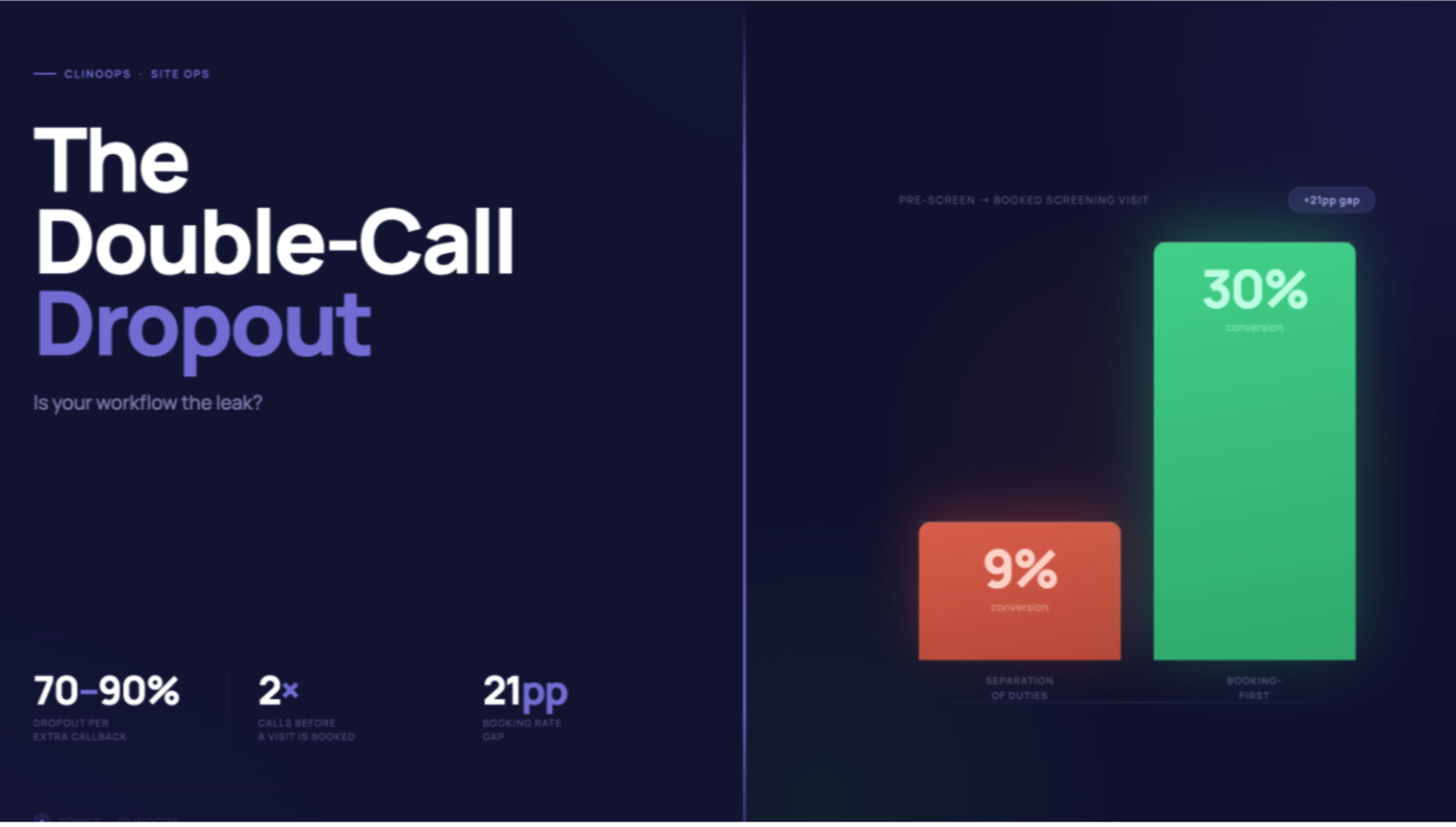
Here's a statistic that should catch the attention of every clin ops leader: 72% of potential trial participants who call a site never make it to a screening visit.
Most sponsors assume this is an eligibility issue. Poor protocol fit. Wrong indication. Natural attrition.
But here's what we're actually seeing when we review site interactions: qualified patients are losing interest during that first phone call... not because of eligibility, but because of how the conversation unfolds.
Where Qualified Patients Quietly Slip Away
Walk into any site and ask the study coordinator what their toughest task is. You'll (typically) hear about source docs, monitoring visits, or data queries.
You won't hear "answering the phone."
Yet that initial phone interaction... the one that happens when a curious patient responds to an ad or gets referred by their physician... might be the highest-stakes 8 minutes of your entire recruitment timeline.
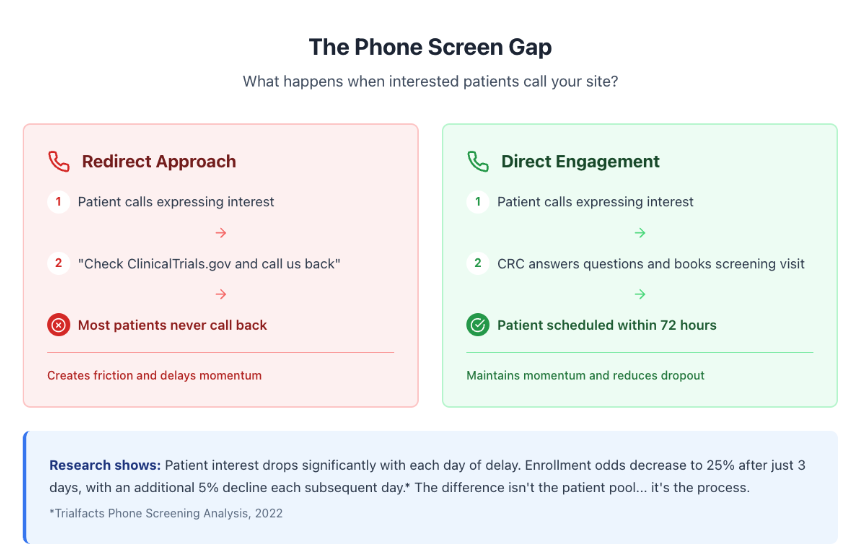
What's actually happening:
- Patient calls expressing interest in the trial
- CRC isn't sure how to assess eligibility verbally
- CRC directs patient to ClinicalTrials.gov to "read more about the study" (yikes!)
- CRC asks patient to call back after reviewing
- Patient never calls back
Sound familiar?
We tracked this pattern across neuroscience trials last quarter. When CRCs redirected callers to external resources, only 18% called back. When CRCs kept the conversation going and scheduled immediately, 64% showed for screening visits.
That's not a small difference. That's the gap between meeting enrollment targets and explaining timeline delays to your executive team.
Why This Isn't Like Sales Training (But Could Learn From It)
Let's address the obvious comparison: In sales, teams use tools like Gong to review calls, identify drop-off points, and train reps on better conversations.
Clinical trials operate under completely different constraints:
- Regulatory requirements around what can and cannot be discussed pre-consent
- Medical accuracy requirements that don't exist in typical sales conversations
- Patient safety considerations that need clinical judgment, not scripting
- Documentation standards that make call recording complex
You can't just implement a simple training playbook and call it done.
What Better Phone Screening Actually Looks Like
The best-performing sites we work with treat phone screening as a trainable skill, not an inherent talent.
They focus on three specific areas:
1. Clear Eligibility Triage (Without Practicing Medicine)
CRCs learn to ask the right questions to quickly assess basic fit:
(Illustrative examples)
- "Can you tell me a bit about your diagnosis and when you were first diagnosed?"
- "Are you currently working with a neurologist or movement disorder specialist?"
- "What medications are you taking for [condition]?"
This isn't diagnosing. It's efficient information gathering within appropriate boundaries.
2. Building Rapport Under Time Pressure
Patients calling about trials are often anxious, confused, or skeptical. The CRC who can create a 3-minute connection... while simultaneously gathering eligibility data and explaining next steps... that's a trained skill.
It requires understanding how to:
- Acknowledge patient concerns authentically
- Explain complex trial concepts in accessible language
- Create urgency around scheduling without being pushy
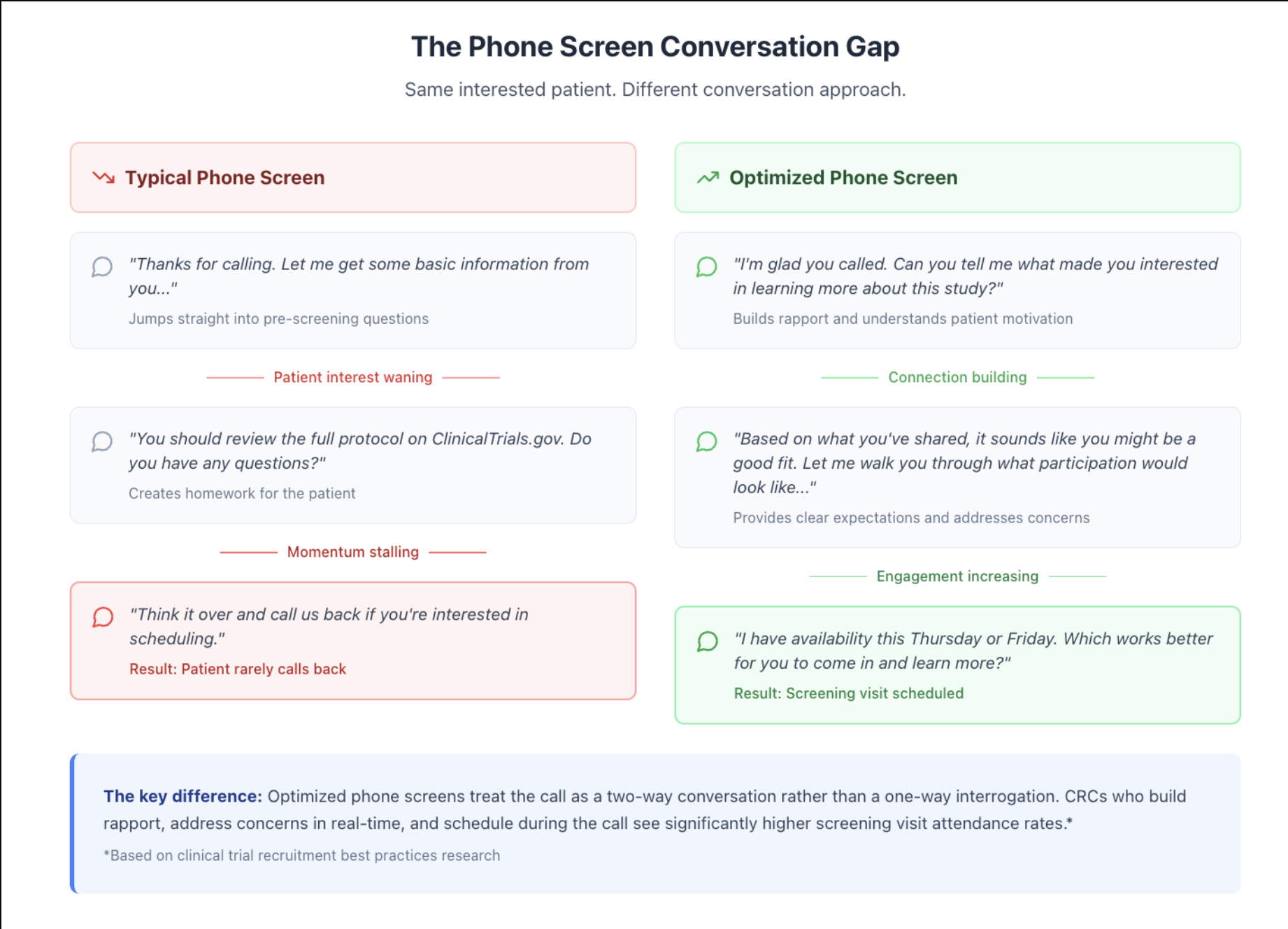
3. Handling the "I Need to Think About It" Moment
This is where most calls die. Patient sounds interested, but hesitant. CRC doesn't want to be aggressive. Call ends with "think about it and call us back."
Trained CRCs handle this differently (illustrative examples):
- "I completely understand this is a big decision. Can I answer any specific questions while I have you?"
- "Would it help to schedule a screening visit where you can meet our team and get all your questions answered in person? There's no commitment at that stage."
- "Many patients find it helpful to bring a family member to learn more together. Would that work better for you?"
The goal isn't manipulation. It's reducing friction for patients who are genuinely interested but uncertain about next steps.
The Training Gap (And Why It Exists)
Sites don't deliberately under-train CRCs on phone skills. The gap exists because traditional CRC training focuses on GCP compliance, protocol procedures, regulatory documentation, and safety reporting — but rarely covers conversational techniques, quick eligibility assessment, handling patient objections, or time management during high-call-volume periods.
This made sense historically. Most trials relied on physician referrals or established patient databases. Phone inquiries from advertising were secondary.
Trials combining digital and traditional recruitment now see 156% more qualified inquiries. Phone screening is a primary conversion point. But training hasn't caught up.
Quick Win: The 15-Minute Call Review Protocol
You don't need sophisticated technology to start improving phone screening outcomes. Start with this:
- Week 1: Have CRCs self-report their 3 most common patient objections or questions during phone screens
- Week 2: Host a 30-minute team session sharing these patterns and workshopping responses together
- Week 3: Create a simple "Phone Screen FAQ" document with approved responses to common concerns
- Week 4: Have each CRC listen to their own calls (if recorded under appropriate consent and regulatory guidelines) or role-play scenarios with another team member
The improvement often shows up in the next enrollment report.
When Technology Actually Helps (And When It Doesn't)
Some sponsors are experimenting with AI-powered tools to support CRC phone training. These can work well for post-call summarization, eligibility flagging, response suggestions, and performance analytics.
What AI can't do: replace the human warmth needed to build trust with anxious patients, make nuanced clinical judgments, handle emotionally complex situations, or navigate the relational aspects of recruiting within patient communities.
Think of technology as a training aid, not a replacement for skilled communication.
What This Means for Your Next Trial
If you're planning a neuroscience trial (or any study where patient-initiated calls are part of your recruitment strategy), add this to your site training:
Before sites activate:
- Create site-specific phone screening guides based on your protocol
- Role-play common patient scenarios during investigator meetings
- Provide example responses to predictable objections ("I'm worried about placebo," "I can't commit to that visit schedule," "My doctor isn't sure about this")
During enrollment:
- Track conversion rates from initial call to scheduled screening
- Review patterns in patient drop-offs (time of day? specific questions? CRC availability?)
- Share high-performing approaches across sites
When enrollment plateaus:
- Before adding more sites or increasing ad spend, audit your phone screening process
- Sometimes the issue isn't awareness... it's conversion
The sites that treat phone screening as a strategic capability are often the top enrollers. Not because they have better patient populations. Because they're capturing the interest that other sites accidentally let slip away.
The bottom line: Your CRCs are already having these phone conversations. The question is whether they're happening by instinct... or by design.
Training doesn't have to be complex. It just has to exist.
Start with one site. Review one week of calls. Identify one pattern to improve.
The patients who are willing to pick up the phone and call your site? They've already done the hard part. Don't lose them in the next 8 minutes.
Want to discuss how to implement systematic phone screening improvements without overwhelming your sites? Reply directly at brandon@withpower.com with your biggest phone screening challenge.